Tennis elbow (often referred to as lateral epicondylopathy, lateral epicondylitis, or lateral epicondylosis) was originally thought to be inflammation of the tendon, bone tendon junction or muscle tendon junction on the outside of the elbow. Runge (1873) is usually credited for the first description of the condition but the term ‘tennis elbow’ first appeared in an 1883 paper by Major called Lawn-tennis elbow.
Recommendation:
- Continuous 1mhz
- 0.8-1.5 W/cm2
- 3-5 mins
- Frequency = 1x per day down to 1 x per week
- Session 5-15 as required
- Combine with =
- Deep friction massage
- Kinesio taping
- Home exercises (Tyler twist)
- Accupuncture
- Bracing (either elbow or wrist)
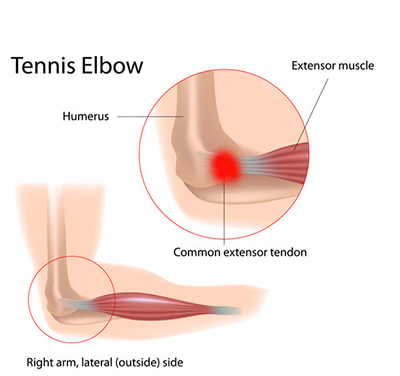
In more recent times the symptoms people suffer has been attributed to degeneration of the extensor tendon of the humeral lateral epicondyle due to microscopic injuries. Common symptoms include pain, tenderness over the lateral epicondyle, pain upon gripping, and ulna deviation (dorsiflexion) against resistance of the wrist, middle finger, or both (Ahmed et al. 2013) .
Conservative treatments such as nonsteroidal anti-inflammatory drugs, local steroid injections, strengthening exercises, stretching, taping, ultrasound, iontophoresis, laser, acupuncture, shockwave and massage are regularly used.
Bisset et al. (2005) performed a review of the literature up to that point which included ultrasound and various combination treatments. In the review only Lundberg et al. (1988) had studied US alone vs. sham US (placebo) they reported significantly improved pain levels in the US group at three months compared with the placebo group.
Davidson et al (2001) compared eight treatment sessions of US and acupuncture and found that, at four weeks follow up, there were significant improvements in all outcome measures for both groups, but that there was no difference between groups.
Stratford et al (1989) used phonophoresis (no drug versus drug) as one factor and transverse friction massage (no frictions versus frictions) as the other. Outcome measures after nine treatment sessions did not support the use of transverse friction massage or hydrocortisone coupling gel, finding no added benefits over that of US alone.
Smidt et al (2002) evaluated a six week combined programme of massage, US, and exercises, and compared this group with a corticosteroid injection group and a wait and see (control) group. At six weeks, there were significant differences between all three groups. The success rate at six weeks between the combined physical intervention and control group was in favour of the intervention and this was maintained at 12 months.
In 2017 Kubot et al. compared the effects of ultrasound and shockwave on lateral elbow pain. They performed 10 sessions of ultrasound (once daily) and looked at pain levels (VAS) and used the Leitinen questionnaire immediately after the end of treatment and at 8 weeks following completion. They found that ultrasound reduced the pain significantly at 8 weeks and was an effective treatment for Tennis Elbow. Of interest the shockwave group did do better overall but the shockwave treatment is more painful during the process.
Lizis (2015) used continuous ultrasound to treat tennis elbow – intensity, 0.8 W/cm2, 1 MHz. The patients received a series of 10 treatments 3 times per week. Lizis found that ultrasound reduced pain in all metrics (except grip strength pain) immediately after treatment and at 3 months, however once again shockwave treatments offered better results.
Shaheen et al. 2019 looked at therapeutic ultrasound and kinesio tape in treatment of tennis elbow. They used 1Mz, continuous, 1.5w/cm, 5 minutes per session, 12 sessions over four weeks, 3 sessions per week. They found therapeutic ultrasound or kinesio taping combined with exercises for four weeks in patients with tennis elbow resulted in significant increase in hand grip strength. A significant decrease in pain intensity occurred in both groups.
What about LIPUS? D’Vaz et al. (2006), assessed the effectiveness of low-intensity pulsed ultrasound therapy (LIPUS) vs placebo therapy daily for 12 weeks in patients with chronic lateral epicondylitis in a randomized, double-blind, placebo controlled trial. In this study LIPUS was no more effective for a large treatment effect than placebo for recalcitrant lateral elbow pain.